
A new era for pancreatic cancer treatment?
Phase 3 results for daraxonrasib are turning heads and raising big questions about where cancer therapy goes next.
Clinical Connections · June 2026 · 5 min read · Source: O'Reilly EM et al. N Engl J Med 2026. DOI: 10.1056/NEJMoa2605555 · By Maria Poimenidou
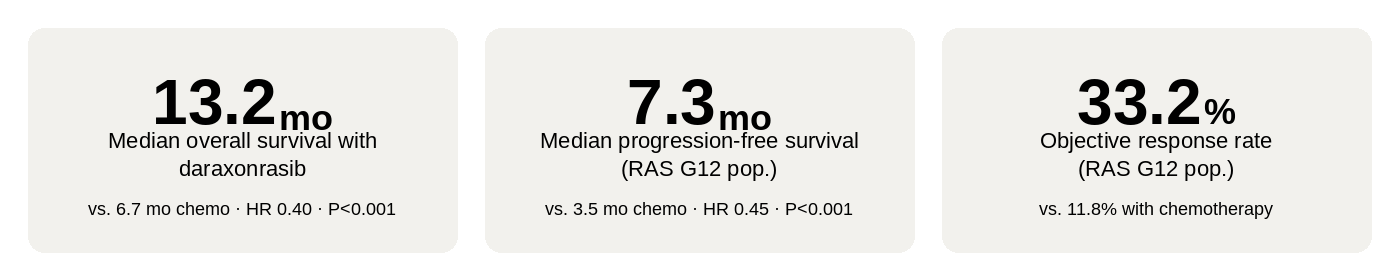
For decades, patients diagnosed with metastatic pancreatic cancer have faced some of the bleakest odds in oncology. Even with the best available chemotherapies, outcomes in the second-line setting have been stubbornly poor: median overall survival of just 6 to 7 months, a response rate in the low teens, and substantial toxicity. Results from the phase 3 RASolute 302 trial, published simultaneously in the New England Journal of Medicine and presented at ASCO 2026, report a 60% reduction in the risk of death with daraxonrasib compared to chemotherapy, a hazard ratio of 0.40 (95% CI, 0.30 to 0.54; P<0.001), and a median overall survival of 13.2 months versus 6.6 months.
The international trial enrolled 500 patients across 59 sites in six countries, all previously treated with one line of chemotherapy for metastatic disease. Patients were randomized 1:1 to receive daraxonrasib at 300 mg orally once daily or investigator-choice chemotherapy. Of those enrolled, 91.8% had RAS G12 mutations, forming the primary analysis population. Survival benefit was consistent across this subgroup and the overall population.
What is daraxonrasib and how does it work?
Over 90% of pancreatic cancers carry oncogenic mutations in the RAS gene family, most commonly at KRAS codon 12. These mutations lock RAS into its active, GTP-bound state, constitutively firing proliferation signals downstream regardless of what the cell actually needs. Think of it as a light switch jammed permanently in the on position, with no way to flip it off from above. Scientists have known for years that targeting this would be consequential. The obstacle has been structural: the active conformation of RAS presents no obvious binding pocket for a small molecule inhibitor, which is why direct inhibition proved so difficult for so long.
Daraxonrasib takes a different approach. Rather than binding RAS directly, it recruits an endogenous intracellular protein called cyclophilin A. The drug and cyclophilin A form a binary complex that clamps onto the active GTP-bound state of RAS and suppresses downstream signalling, using the cell's own machinery as part of the inhibitory mechanism. Because it targets the active conformation rather than a specific mutation site, it is effective across KRAS, NRAS, and HRAS, and across G12, G13, and Q61 variants. This broad activity explains the consistent survival benefit seen across RAS mutational subgroups in the trial, and even in the small subset of patients with no identifiable RAS mutation, who may still be RAS-pathway dependent through upstream or downstream alterations.
“It’s been incredibly hard to drug that mutation. That mutated protein is like a round ball, and you just can’t get the drug to stick to it. It’s only through some really amazing chemistry work that scientists have been able to develop a drug to work on it.”
How does it compare to chemotherapy in practice?
Patients in the daraxonrasib arm stayed on treatment for a median of 6.2 months, compared with 1.5 to 3.2 months across the chemotherapy regimens, yet still came out ahead on serious toxicity metrics. Grade 3 or higher treatment-related adverse events occurred in 43.6% of daraxonrasib patients versus 57.5% on chemotherapy. Serious treatment-related adverse events were reported in 10.8% versus 18.7%, and treatment discontinuation due to adverse events was 1.2% versus 11.2%.
The side-effect profile skews dermatological and gastrointestinal rather than haematologic. Rash (85.5%), diarrhoea (58.1%), stomatitis (53.1%), nausea (46.5%), and vomiting (36.9%) were the most common treatment-related events. Chemotherapy produced more fatigue, anaemia, neutropenia, thrombocytopenia, and peripheral neuropathy. On patient-reported outcomes, time to deterioration in pain was 9.0 months with daraxonrasib versus 3.7 months with chemotherapy, and time to deterioration in global health status was 5.6 versus 2.4 months. In a population where symptom burden is often severe from diagnosis, those differences carry real weight.
What comes next
The FDA has granted daraxonrasib fast-track designation and, as of May 2026, permitted Revolution Medicines to begin an expanded access programme, meaning eligible patients with previously treated metastatic disease can access the drug outside of a clinical trial. RASolute 303 is now evaluating daraxonrasib as potential first-line therapy, with or without chemotherapy. Revolution Medicines has three additional RAS inhibitors in clinical development, with a fourth set to begin trials later this year.
“Pancreas cancer may be the first for this drug, but there will be others. Now the floodgates open.”
FOOD FOR THOUGHT
-
KRAS mutations are not unique to pancreatic cancer. They drive tumour growth in lung, colorectal, ovarian, endometrial, and certain bile duct cancers too. Because daraxonrasib targets the active conformation of RAS rather than a mutation-specific site, the mechanism is broadly applicable. Researchers are already asking whether these results in pancreatic cancer open the door to trials in those settings, and the early signals are encouraging. Pancreatic cancer is the start and almost certainly not the final destination.
-
Tumours will eventually develop resistance, as they do with every targeted therapy, and the field is already preparing for that. Revolution Medicines has three additional RAS inhibitors in clinical trials, with a fourth due to start later this year. The goal is an arsenal of agents that clinicians can sequence as resistance emerges. That is a realistic and exciting trajectory, and one that positions RAS inhibition as a durable long-term strategy rather than a single moment in time.
Source: NBC News
-
If daraxonrasib proves effective as a second-line agent, should it eventually be moved to first-line? The authors note, with appropriate caution, that previous randomized first-line trials including FOLFIRINOX, gemcitabine plus nab-paclitaxel, and NALIRIFOX achieved median overall survivals of 8.5 to 11.1 months. Daraxonrasib, used in previously treated patients, achieved 13.2 months. That is a striking comparison, and it makes the ongoing RASolute 303 trial, which is evaluating daraxonrasib as first-line therapy, feel less like a speculative follow-up and more like the next logical and necessary step. If those results hold, treatment algorithms for metastatic pancreatic cancer could look very different within a few years.
Source: O’Reilly EM et al., N Engl J Med 2026 / Dana-Farber press release
-
Access and affordability will matter enormously. Novel targeted therapies often carry significant price tags. The expanded access program approved by the FDA in May 2026 is an encouraging first step toward broader patient access. The bigger picture, though, is that if daraxonrasib eventually proves effective across multiple cancer types with high RAS mutation prevalence, the eligible population becomes very large. There is real opportunity here to get an effective, orally administered, well-tolerated therapy into the hands of patients who need it most. Making sure pricing and coverage decisions reflect that opportunity, rather than limiting it, will be one of the more important conversations that follows approval.